Primary Assessment: How to Quickly Identify Life-Threatening Conditions
Author:
CPR Select Editorial Team
Last updated:
12/9/2025
Primary assessment is the first step in evaluating a patient to identify and prioritize immediate life threats. It involves quickly checking responsiveness, airway, breathing, circulation, and whether emergency services need to be activated.
This structured approach guides responders toward the most critical lifesaving actions. By focusing on immediate threats to oxygenation and perfusion, primary assessment ensures that care starts in the right order during the first crucial minutes of an emergency.
What Is the Primary Assessment?
The primary assessment is a rapid check used in emergency situations to spot life-threatening conditions fast. It’s part of emergency triage and helps clinicians decide what needs to happen right now. The goal is simple: recognize the most urgent problems and act quickly.
Why the Primary Assessment Matters?
In emergencies, every second counts. The primary assessment gives clinicians a quick, focused scan to identify what needs immediate attention. It helps them sort out the most serious physiologic threats and set priorities in the first moments of patient contact, before moving on to any detailed tests or diagnostics.
This assessment zeroes in on conditions that can cause death within minutes and saves everything else for later. It checks for:
A clear and protected airway (including cervical spine protection)
Adequate breathing and ventilation
Effective circulation and severe bleeding
Life-threatening issues like tension pneumothorax, open chest wounds, cardiac tamponade, massive hemorrhage, or airway compromise
By staying focused on these critical areas, responders can act fast and avoid losing valuable time.
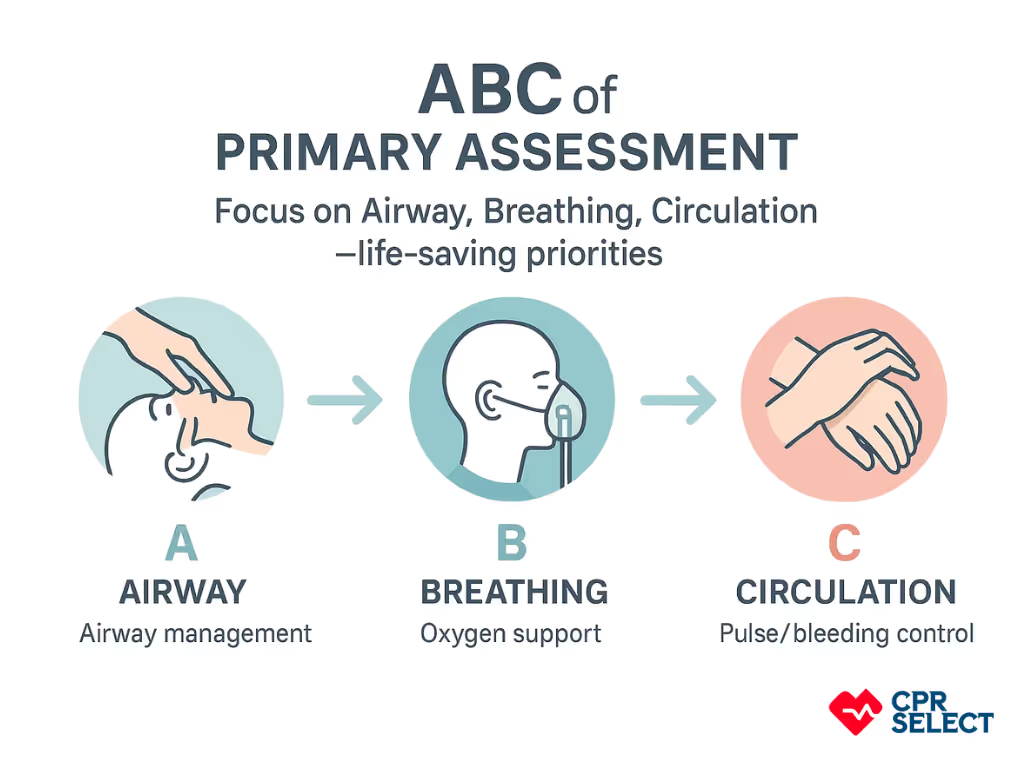
How the ABCs Fit Into the Assessment?
The primary assessment works hand in hand with the ABCs—airway, breathing, and circulation. These steps turn the rapid scan into concrete actions:
Airway: Check and protect the airway, including the cervical spine
Breathing: Watch chest movement, ventilation, and respiratory rate
Circulation: Check pulses, skin color, capillary refill, and control bleeding
These same principles apply to all patients, with slight variations for pediatric and older adults.
Airway
The airway ensures that oxygen can reach the lungs and prevents aspiration. Clinicians check for obstruction, altered consciousness, or trauma, then choose the right intervention. This may include simple maneuvers like the head-tilt chin-lift or jaw thrust (if cervical spine injury is suspected), or advanced airway placement such as endotracheal intubation or a supraglottic airway.
Breathing
Breathing focuses on effective chest movement and gas exchange. Clinicians assess rate, depth, effort, and oxygen saturation, then provide support as needed: supplemental oxygen, high-flow nasal cannula, non-invasive ventilation, or assisted ventilation with a bag-valve-mask when breathing is inadequate.
Circulation
Circulation reflects cardiac output and tissue perfusion. This includes pulse rate and quality, skin temperature, capillary refill, and blood pressure. Interventions may involve IV or IO fluids, vasopressors, and hemorrhage control, depending on the cause of instability.
How the ABCs Differ by Age Group
The ABC priorities stay the same for adults, children, and infants, but the signs and normal ranges differ:
Adults have larger airways and more cardiovascular reserve, so they may maintain blood pressure until late in shock.
Children often compensate with tachycardia and vasoconstriction before developing hypotension.
Infants have narrow airways and respiratory rates around 30–60 breaths per minute, making them more prone to obstruction and rapid decompensation.
These differences change how clinicians interpret findings during the assessment.
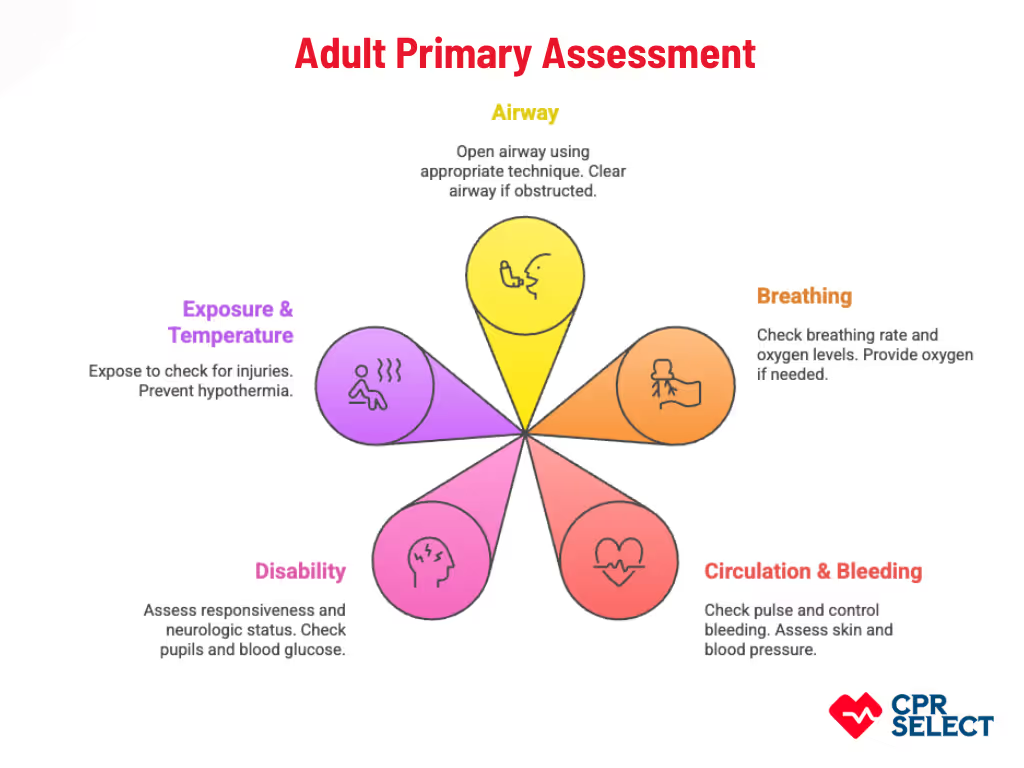
Adult Primary Assessment
The adult primary assessment is a fast, structured check used to spot life-threatening conditions in unresponsive or critically ill adults. You’ll see this done in places like homes, public areas, ambulance scenes, or emergency departments. It follows a clear, step-by-step flow so responders can act quickly and confidently using basic equipment like PPE, airway tools, a bag-valve mask, and an AED.
At its core, the goal is simple: find what can kill the patient right now and fix it first. Adults often have unique risks: chronic illnesses, age-related changes, or medications like blood thinners, so responders must work fast while keeping these factors in mind.
Airway: Open airway (jaw-thrust if neck injury suspected, head-tilt chin-lift if safe); insert oropharyngeal airway if unresponsive with no gag; airway clear when air moves freely or noisy breathing improves; call for advanced airway help if obstruction persists or trauma complicates basic techniques.
Breathing: Check chest rise, respiratory rate, and oxygen levels; provide high-flow oxygen or two-person BVM if inadequate; target SpO₂ 94–98% (most adults), 88–92% (COPD per protocol); watch for tension pneumothorax and follow decompression guidelines if suspected.
Circulation & Bleeding: Check central pulse, assess major bleeding; control bleeding with direct pressure or tourniquet (5–7 cm above wound); assess skin signs, capillary refill, blood pressure; establish IV/IO for shock; escalate to advanced care for hypotension, pulselessness, or worsening mental status.
Disability (Neurologic Status): Assess responsiveness with AVPU or GCS; check pupils; measure blood glucose if altered; treat hypoglycemia per protocol; consider advanced airway if GCS ≤ 8 and airway not protected.
Exposure & Temperature: Briefly expose to check hidden injuries; prevent hypothermia with blankets or warmed IV fluids; document major wounds, deformities, or medical IDs; arrange rapid transfer for severe injuries.
Follow the ABC order, but overlap tasks when more responders are available. For example, one person can manage the airway while another controls bleeding. If any step shows signs of imminent deterioration, activate advanced life support immediately.
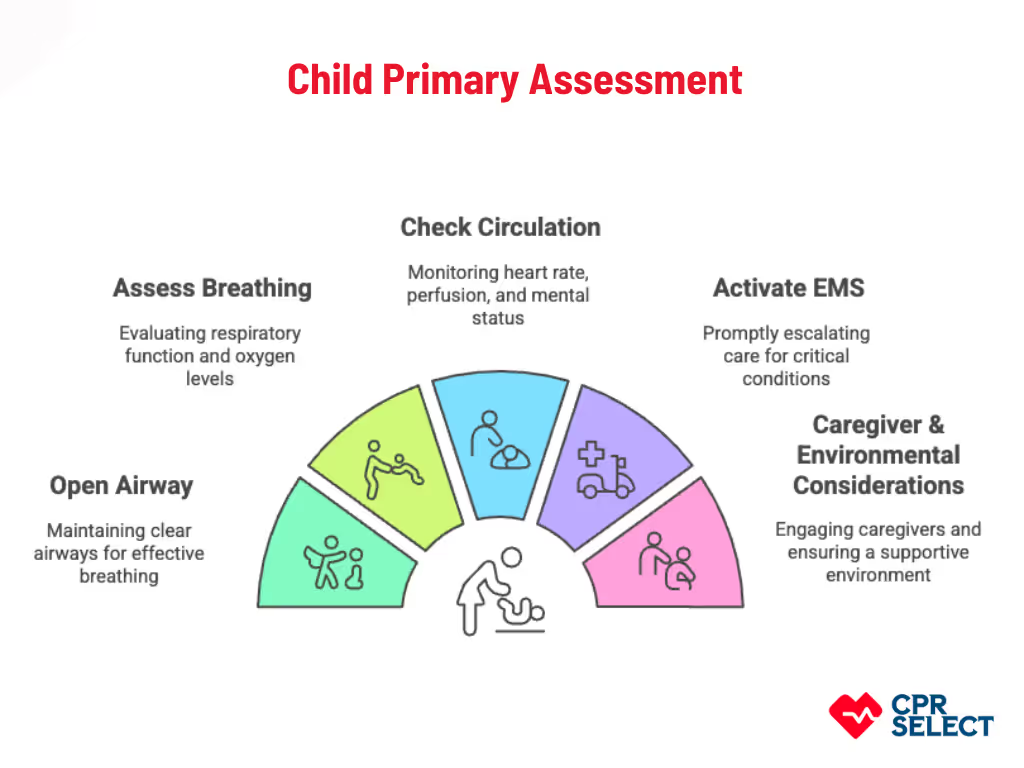
Child Primary Assessment
When a child is critically ill or unresponsive, early recognition of life-threatening conditions can save lives. The child primary assessment is a focused, age‑adjusted evaluation that prioritizes airway, breathing, and circulation while accounting for pediatric anatomy, physiology, and behavior. Children are not just “small adults”, their smaller airways, faster breathing, lower blood volume, and unique developmental responses require special attention.
Check Responsiveness: Determine if the child is alert, responds to voice, or responds only to pain. Use age-appropriate behavioral cues and involve caregivers to guide assessment.
Open Airway: Maintain neutral neck alignment in infants; avoid excessive head tilt in young children. Use jaw-thrust for suspected cervical injury. Select airway adjuncts based on age or weight; prepare suction and escalate to BVM if ventilation is inadequate.
Assess Breathing: Evaluate chest movement, respiratory rate, and oxygen saturation. Watch for nasal flaring, retractions, grunting, or early fatigue. Provide supplemental oxygen when oxygen levels or effort are inadequate.
Check Circulation: Assess pulses (brachial in infants, radial in older children), skin perfusion, capillary refill, and mental status. Use blood pressure only if perfusion assessment is inconclusive. Recognize age-specific heart rates and perfusion thresholds.
Activate EMS: Escalate quickly for respiratory distress, poor perfusion, or altered consciousness. Provide a clear handoff to EMS including the child’s weight, airway interventions, oxygen therapy, medications, and caregiver input.
Caregiver & Environmental Considerations: Engage caregivers for baseline history and behavioral insight. Use familiar objects, gentle handling, and keep the child near caregivers when possible. Ensure pediatric-appropriate airway and oxygen equipment is ready.
The child primary assessment is a rapid, structured approach designed to identify life-threatening conditions quickly while accounting for pediatric differences. Following these steps ensures timely interventions, reduces risk of deterioration, and guides escalation to advanced care. Understanding how pediatric assessment differs from adults helps responders act confidently and safely in critical situations.
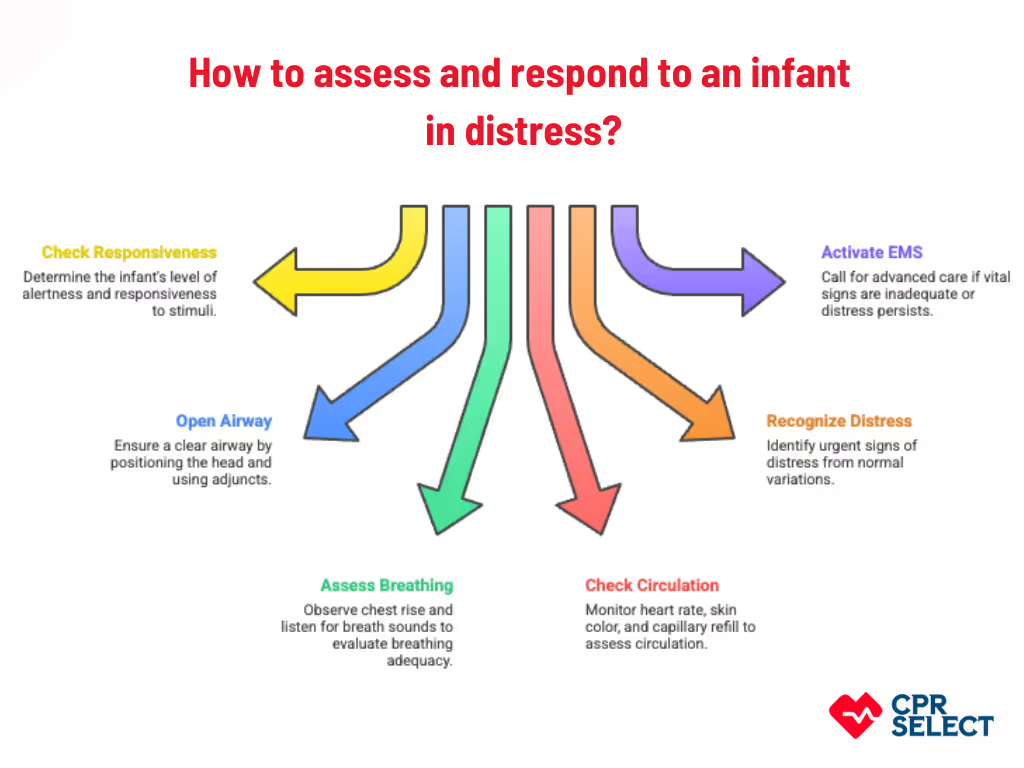
Infant Primary Assessment
The infant primary assessment is a rapid, prioritized evaluation designed to identify immediate life threats and guide interventions tailored to infants’ unique physiology, small size, and limited physiological reserve. Infants are not small children—airway anatomy, breathing patterns, circulation dynamics, and fragile tissues require age-specific assessment techniques.
Check Responsiveness: Gently stimulate the infant to see if they are alert, responsive to voice, or responsive only to pain. Use age-appropriate cues and avoid rough handling.
Open Airway: Position the head in a neutral or slight sniffing position; avoid full head tilt. Account for the larger occiput, high larynx, and relatively large tongue. Use appropriately sized airway adjuncts, and suction nasal secretions if needed.
Assess Breathing: Observe chest rise, nasal patency, and audible breath sounds. Recognize that agonal gasps are ineffective. Provide supplemental oxygen or bag-valve-mask ventilation if breathing is inadequate.
Check Circulation: Focus on heart rate, capillary refill, skin color, and perfusion. Use two-finger compressions for single rescuers or two thumb encircling technique for two rescuers if CPR is required. Avoid excessive force due to compliant infant chest walls.
Recognize Distress vs. Normal Variations: Watch for nasal flaring, retractions, grunting, pallor, cyanosis, poor feeding, lethargy, or abnormal cry. Distinguish urgent signs from normal mimics such as brief periodic breathing, transient acrocyanosis, or startle-related apnea in preterm infants.
Activate EMS and Escalate Safely: Call for advanced care when airway, breathing, or circulation is inadequate, heart rate is <60 bpm despite support, or shock signs persist. Limit invasive attempts and prioritize rapid transfer to advanced care.
Caregiver & Environmental Considerations: Engage caregivers for baseline information, provide comfort with familiar objects, and ensure appropriate infant-sized equipment is ready.
The infant primary assessment emphasizes rapid identification of life-threatening conditions while accounting for infants’ unique anatomy, physiology, and fragility. Following these steps ensures timely interventions, minimizes harm, and guides escalation to advanced care. Understanding the differences between infants, children, and adults helps responders act confidently and safely in critical situations.
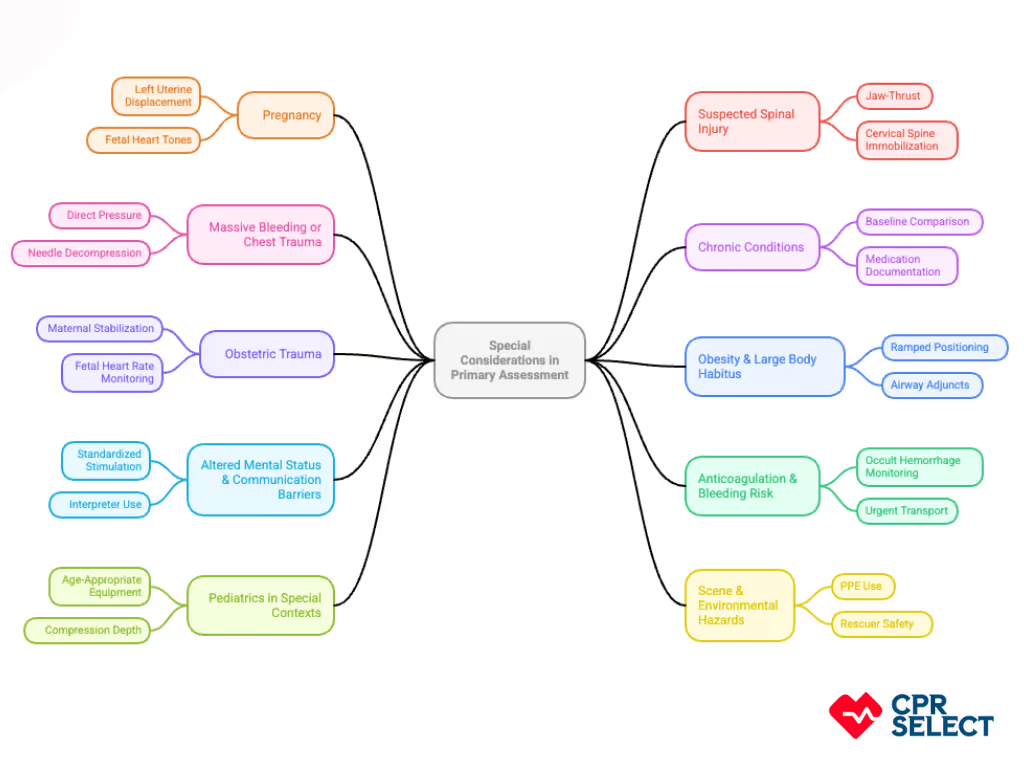
Special Considerations in Primary Assessment
Special considerations in primary assessment are important because they alter physiology, increase risk, and require adaptations to standard adult, child, or infant ABC steps. Adjustments preserve airway, breathing, and circulation while avoiding condition-specific harm and preventing iatrogenic injury. Key special considerations include:
Pregnancy: Prioritize left uterine displacement (15–30° tilt or manual push) to reduce aortocaval compression. Maintain airway access, monitor maternal SpO₂ ≥95%, and palpate femoral or carotid pulses. Escalate to obstetric-capable transport if maternal hypotension or absent fetal heart tones occur.
Suspected Spinal Injury: Use jaw-thrust with manual inline stabilization for airway. Avoid head tilt unless ventilation is inadequate. Employ two-rescuer BVM technique and immobilize cervical spine without delaying life-saving airway interventions.
Massive Bleeding or Chest Trauma: Control life-threatening hemorrhage with direct pressure or tourniquet and perform needle decompression for tension pneumothorax if within scope. Reassess ABCs after interventions and activate EMS for advanced care.
Chronic Conditions: Adjust assessment for cardiac disease, COPD, diabetes, anticoagulation, pacemakers, or implanted devices. Compare current vitals to baseline, lower thresholds for escalation, and document medications and oxygen use.
Obstetric Trauma: Prioritize maternal stabilization, maintain left uterine displacement, and monitor fetal heart rate ≥20 weeks gestation when possible. Escalate immediately for hypotension, vaginal bleeding, or abnormal fetal heart rate.
Obesity & Large Body Habitus: Use ramped positioning, select appropriate airway adjuncts, check femoral or carotid pulses, anticipate ventilation difficulties, and consider early video laryngoscopy or multiple personnel for airway and movement.
Altered Mental Status & Communication Barriers: Apply standardized stimulation (loud voice, sternal rub), gather bystander history, use interpreters if needed, and check glucose for hypoglycemia. Assume reduced airway protection until verified.
Anticoagulation & Bleeding Risk: Watch for occult hemorrhage, expanding hematomas, or subtle perfusion changes. Lower threshold for aggressive bleeding control and urgent transport. Communicate anticoagulant type and last dose for reversal planning.
Pediatrics in Special Contexts: Modify standard child assessment for chronic illness, congenital anomalies, or trauma. Use age-appropriate equipment, adjust compression depth, ventilation volumes, and respond quickly to heart rate <60 in infants with poor perfusion.
Scene & Environmental Hazards: Assess for fire, toxins, electrical hazards, or structural instability. Use PPE, minimize exposure, and prioritize rescuer safety alongside patient ABCs. Activate EMS for hazardous conditions.
Special considerations guide how ABCs are applied without replacing them. They require heightened vigilance, age-specific adjustments for adults, children, and infants, and prompt EMS activation. Ongoing training ensures clinicians can safely integrate these adaptations into real-life primary assessments.
How BLS Certification Prepares You
BLS certification prepares responders to perform rapid, structured primary assessments for adults, children, and infants by building knowledge, decision-making frameworks, and essential non-technical skills like communication and teamwork. Learners gain age-specific understanding of airway, breathing, and circulation priorities, recognizing subtle signs of distress such as respiratory compromise in children, poor feeding in infants, and altered mental status in adults. The course emphasizes adaptive decision-making under time pressure, coordination with bystanders and EMS, standardized handover reporting, and awareness of legal and ethical considerations. By integrating these elements, CPR Select enhances responder confidence, assessment speed, and accuracy, clarifies the limits of basic interventions, and underscores timely escalation to advanced care when necessary.
Get CPR Certified in Minutes for as low as $19.95
Join thousands of professionals that have been certified online with us
Do the steps change by age and should I follow the same assessment for adults, children, and infants?
The core goals of airway, breathing, circulation, and disability remain the same across all ages, but techniques and equipment vary. Adults and children typically use a head-tilt chin-lift unless a spinal injury is suspected, while infants require a neutral head position and gentle support. Ventilation devices and compression depths are also age-specific: adults need deeper compressions, children use about one-third of chest depth, and infants require gentle two-thumb or two-finger compressions.
How long should the primary assessment take in an emergency and what timing should I expect?
The initial life threat check should take no more than 60 seconds. Rapidly prioritize airway, breathing, and circulation over secondary tasks. Following this quick approach ensures timely interventions and immediate escalation when life threats are identified.
What should I do differently if the patient is pregnant or has suspected major trauma?
In pregnancy, left uterine displacement reduces aortocaval compression, and you should anticipate airway challenges such as edema or aspiration risk. For major trauma, spinal motion restriction is critical; secure the airway with manual inline stabilization or a cervical collar while addressing life-threatening bleeding. The primary goal remains identifying immediate threats and stabilizing the patient quickly.
When should I activate EMS instead of continuing on-scene care and how do I decide quickly?
Activate EMS immediately if there is an unsecured airway, absent or inadequate breathing, severe uncontrolled bleeding, or unstable circulation. Early activation is also recommended for unresponsive patients, suspected stroke or heart attack, and major trauma. Prompt escalation ensures the patient receives definitive care without delay.
Which common mistakes should I avoid during the primary assessment?
Common mistakes include hesitating to act, focusing on noncritical details, skipping vital reassessments, or neglecting rapid airway and breathing checks. To correct these, follow a structured ABCD sequence, assign clear roles, use checklists, and practice scenarios regularly to improve speed and accuracy.
What is a secondary assessment and when should I perform it?
A secondary assessment is a more detailed evaluation performed after the primary assessment and stabilization of immediate life threats. It includes a full head-to-toe exam, vital signs, patient history (SAMPLE), and identification of injuries or conditions not immediately life-threatening. Perform secondary assessment only once airway, breathing, and circulation are secure, and adjust your approach based on patient age, condition, and the presence of trauma or chronic illnesses.