Asthma First Aid: Recognizing and Managing an Asthma Attack
Author:
CPR Select
Last updated:
9/1/2025
Asthma is a chronic respiratory condition marked by airway inflammation and reversible airflow limitation, and early recognition with quick action reduces the risk of deterioration and improves outcomes. While routine symptoms are common, they quickly escalate into a severe asthma attack, especially if recognition or treatment is delayed.
Severe attacks develop over minutes to hours, with peak expiratory flow below 50% signaling high risk, according to the National Asthma Education and Prevention Program. Early recognition and prompt action improve outcomes.
This article will cover triggers, signs and symptoms, first aid, inhaler technique, when to call emergency services, prevention, training, and FAQs, with a focus onclear, actionable steps for patients, caregivers, and the public.
What is an Asthma Attack?
An asthma attack is an acute episode of airway narrowing that causes sudden shortness of breath, wheezing, and reduced airflow. It arises from the underlying chronic condition of asthma, which involves persistent airway inflammation, hyperresponsiveness, mucus overproduction, and structural changes. Poorly controlled asthma, defined in international guidelines as frequent daytime symptoms, nighttime awakenings, use of a rescue inhaler more than twice a week, or two or more steroid-requiring exacerbations in a year, increases both the frequency and severity of attacks.
How Asthma Attacks Happen?
An attack begins when a trigger provokes bronchospasm, airway swelling, and mucus plugging. Common triggers include viral infections, allergens such as dust mites, pollen, and animal dander, tobacco smoke, strong odors, fumes, cold air, exercise, and certain medications like NSAIDs or beta blockers in susceptible individuals. These reactions raise airway resistance and limit expiratory flow, producing rapid breathlessness.
Severe asthma attacks can become life-threatening within minutes to hours. Without prompt treatment, attacks can lead to hypoxemia, carbon dioxide retention, and respiratory failure.
Why Early Recognition Matters?
Asthma attacks can be mild and short, getting better quickly with inhaled short-acting beta agonists. Or they can be severe and long, needing nebulized medicine, steroids, oxygen, and emergency care. Understanding their nature and link to chronic asthma highlights the importance of trigger avoidance, rapid recognition, and early intervention.
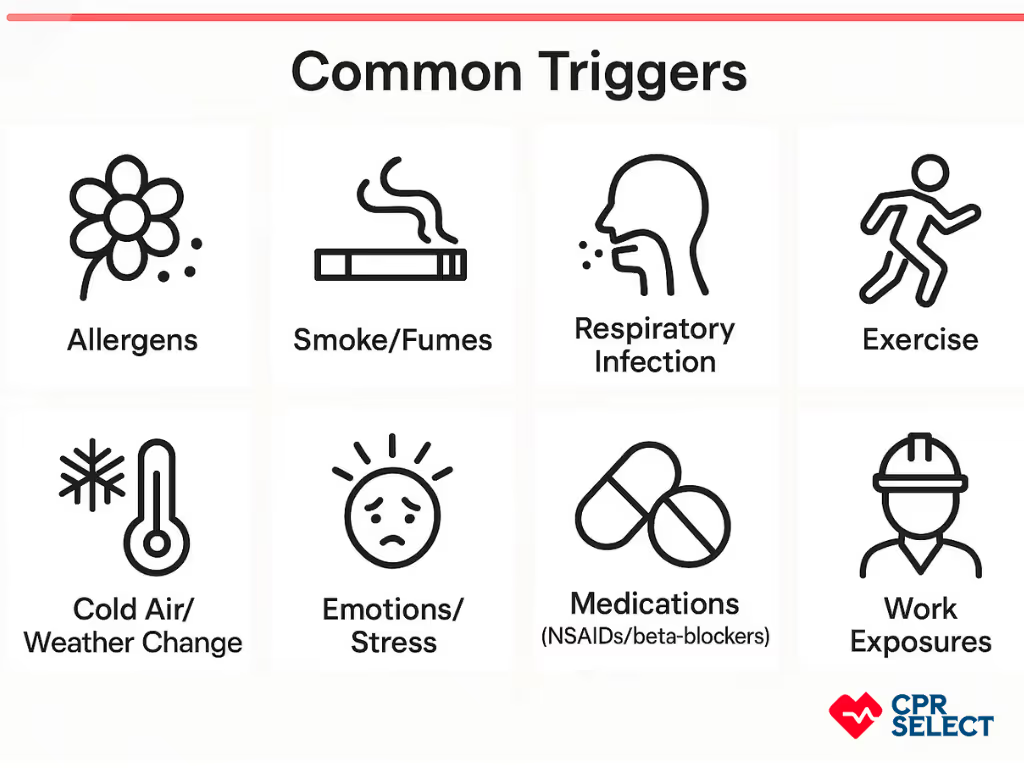
What are the Common Triggers of Asthma Attacks?
Common triggers of asthma attacks include allergens, irritants, infections, exercise, environmental changes, emotions, medications, occupational exposures, and mixed causes. Recognizing these helps with prevention and first aid.
Allergens: Dust mite feces, pet dander, mold, and pollens can inflame airways through immune reactions. This causes bronchoconstriction, mucus buildup, and wheezing. Knowing allergen types and seasonal patterns supports avoidance and medication adjustment.
Irritants: Tobacco smoke, wood smoke, vehicle exhaust, cleaning fumes, and chemicals can irritate airways and cause bronchospasm.
Respiratory Infections: Viruses like rhinovirus and influenza can worsen airway inflammation and trigger attacks.
Exercise and Physical Exertion: Running, cycling, or similar activities can cool and dry airways, triggering symptoms. Attacks often start within 10–15 minutes, according to the American Academy of Allergy, Asthma & Immunology (AAAAI).
Weather and Environmental Changes: Cold air, humidity shifts, barometric pressure changes, and “thunderstorm asthma” can trigger attacks.
Strong Emotions and Stress: Stress and strong emotions can trigger bronchospasm through hyperventilation.
Medications and Substances: Beta-blockers, aspirin, some NSAIDs, and contrast agents can cause attacks in sensitive people.
Occupational Exposures: Flour dust, isocyanates, animal proteins, and cleaning products can cause work-related asthma.
Attacks often have more than one cause. Tracking symptoms and peak flow helps identify patterns and guide personalized action plans.
What are the Signs and Symptoms of an Asthma Attack?
Below are the observable signs and symptoms that typically occur during an asthma attack:
Shortness of breath: Breathing fast, shallow, or deep, with visible chest movement.
Wheezing: A high-pitched whistling sound when breathing out, often heard without a stethoscope.
Fast breathing and muscle use: Breathing rate increases, and neck or chest muscles may visibly tighten. You might see skin pulling in above the collarbone or between the ribs.
Difficulty speaking: The person may pause often to catch their breath or speak only a few words at a time.
Posture changes: Leaning forward with hands on knees or a chair, nasal flaring, or tight lips to ease breathing.
Severe signs: Blue lips or skin (cyanosis), pale skin, sweating, confusion, or drowsiness, which signal low oxygen and a serious emergency, according to the American Lung Association.
Recognizing the signs enables rapid identification of an asthma attack and guides urgent assessment. The next section, First Aid for an Asthma Attack, presents immediate response measures once readers have identified the severity and presence of an acute episode.
First Aid for an Asthma Attack
This first aid guide covers immediate, short term first aid for an ongoing asthma attack and does not replace professional medical treatment or long term management plans. The scope focuses on rapid actions to relieve airway obstruction and maintain ventilation in the minutes that follow onset. Helpers should confirm responsiveness, check for the person’s prescribed quick relief medication and device, and note any known allergies or recent changes in health before proceeding.
Assess breathing and alertness
Help administer quick relief medication
Position to ease breathing and calm
Monitor response and escalate if no improvement; watch for danger signs.
Escalate to emergency care immediately. Report observations.
1. Assess breathing and alertness
Assess breathing and alertness by observing respiratory rate, chest and abdominal effort, ability to speak in sentences, skin color, and level of distress, and by checking airway patency and obvious environmental hazards.
Count breaths for 30 seconds to estimate respiratory rate. Ask the person to say a short sentence to judge speech ability, and look for use of neck or chest accessory muscles and nasal flaring as signs of increased work of breathing.
Rapid assessment of respiratory status is critical in asthma emergencies. According to the Global Initiative for Asthma (GINA) guidelines, early detection of worsening symptoms allows timely bronchodilator use and emergency escalation, which can help prevent respiratory failure.
2. Help administer quick relief medication
Help give quick relief medicine by finding the patient's inhaler or nebulizer. Make sure the device is ready. Help the patient use a spacer or mouthpiece if they have one. Make sure the patient breathes in with each spray or dose.
If using a metered dose inhaler with spacer, give one to two puffs and wait 20 to 60 seconds between puffs, then reassess
If no spacer is available, instruct the person to exhale fully, place the inhaler in the mouth, actuate once and inhale slowly and deeply, hold breath for up to 10 seconds if tolerated, then repeat per the person’s action plan up to a usual maximum of 3 to 10 puffs depending on the plan.
For nebulizer use, run the standard nebulization of salbutamol 2.5 mg in 2.5 to 5 mL saline or as prescribed. Observe timing by allowing a few minutes for clinical response after inhalation and consider repeating per the person’s established plan or emergency guidance if symptoms persist.
Avoid giving medicines that are not prescribed to the patient.
3. Position to ease breathing and calm
Position to ease breathing and calm the patient by seating the person upright with shoulders supported and leaning slightly forward if that reduces effort, and by offering steady reassurance and guided slow breaths to lower panic and improve ventilation.
Encourage the person to sit facing forward with elbows resting on knees or a table to help accessory muscles work more effectively; do not force breathing techniques that increase hyperventilation. Avoid laying the person flat if it increases the work of breathing, and monitor closely to see whether the chosen position reduces respiratory rate and accessory muscle use or instead worsens distress.
4. Monitor response and repeat if necessary
Watch the patient's breathlessness, speech, breathing rate, and skin color for signs of improvement within minutes after treatment. If there is no clear improvement, give the quick relief medicine again as the patient's plan or emergency guidelines say.
Use a pulse oximeter if available; oxygen saturation less than 92 percent in adults or a falling trend requires urgent escalation. Watch for danger signs such as inability to speak more than a few words, exhaustion, confusion, or a silent chest where breath sounds are markedly reduced.
Non response signs such as increasing drowsiness, falling oxygen saturation, silent chest, or worsening cyanosis indicate the need to escalate beyond first aid.
5. Escalate to emergency care when needed
Call emergency services right away if the patient stays very distressed or gets worse. Keep watching the patient and help with the inhaler or nebulizer while waiting. Get ready to give clear information to the emergency responders.
Report critical observations such as duration of attack, number of inhaler doses given, changes in consciousness, breathing rate, and oxygenation; do not delay contacting emergency services when danger signs are present.
If the person’s own action plan instructs to call emergency services after a specified number of puffs or minutes without improvement, follow that plan.
Special Considerations: Age and Health Conditions
Unconscious patients need immediate emergency care. Always check the airway first. Airway protection and ventilation differ from conscious first aid.
If the person cannot use an inhaler, escalate quickly. Medication delivery will be delayed.
If there is no prescribed inhaler, call for medical help immediately. Do not give unfamiliar drugs. These may cause allergic or adverse reactions.
Heart disease or pregnancy may change how the body responds. Seek professional evaluation promptly to ensure safe care.
Children and infants may show different signs. Watch for irritability, poor feeding, and retractions. Use the prescribed age-appropriate dose and device. Seek help sooner for young children.
The main goal is to stabilize breathing, relieve symptoms, and obtain help if necessary. Correct inhaler technique is essential for opening the airways. Knowing the right technique makes the first aid steps more effective.
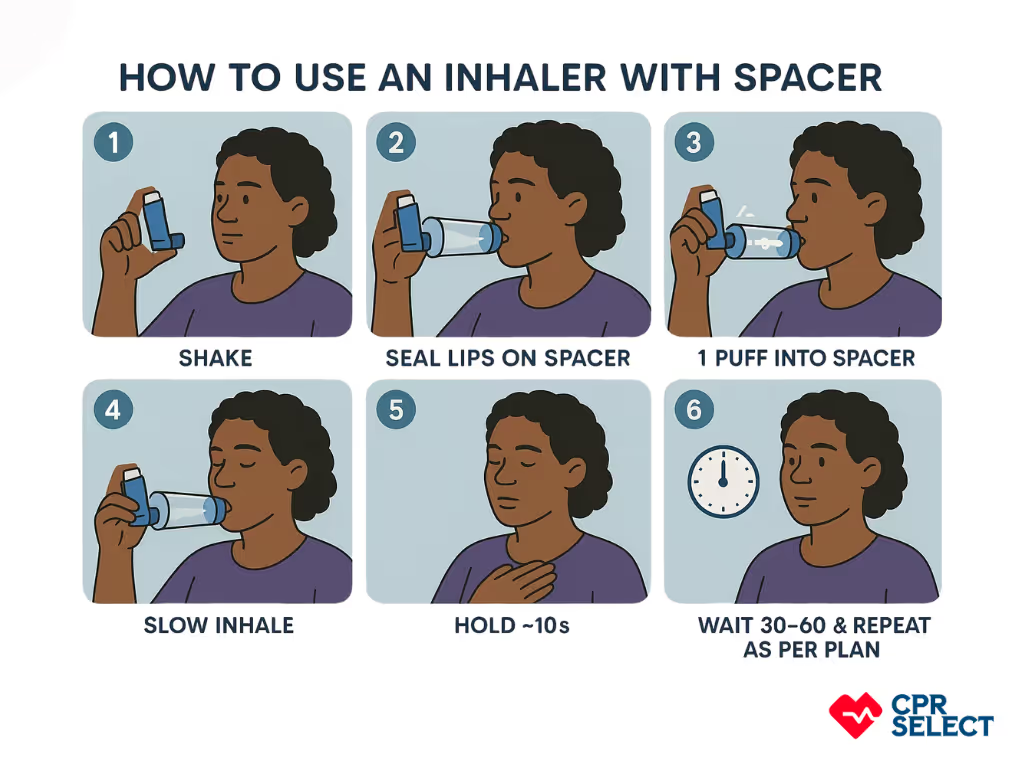
How to Use an Asthma Inhaler Properly?
Using an inhaler correctly helps medicine reach the airways and quickly reduce narrowing. This applies to pressurized metered dose inhalers (MDIs) and to spacers. The steps below focus on using quick-relief medication during an asthma attack.
Prepare the inhaler: Check the dose counter. Shake the inhaler 5–10 times if required. Remove the cap. If unused for a week or more, spray 1–2 test puffs into the air to prime it. This makes sure the correct dose is delivered.
Sit upright and breathe normally: Sit upright in a chair. Take 2–3 normal breaths before using the inhaler. This helps open the airways so the medicine can travel deeper into the lungs.
Breathe out fully: Breathe out away from the mouthpiece until your lungs feel comfortably empty. This gives you more space to inhale the medicine deeply.
Inhale and press: Place the mouthpiece in your mouth and seal your lips around it. Start breathing in slowly and deeply. Press down on the canister once as you inhale. Continue breathing in for 4–6 seconds. If using a spacer, press once into the spacer, then inhale slowly. With large spacers, you can take 5–6 normal breaths instead of one deep breath.
Hold your breath: Hold your breath for about 10 seconds, or as long as is comfortable. This allows the medicine to settle in the airways.
Wait and repeat if needed: Wait 30–60 seconds before taking another puff. Repeat up to the number of puffs in your asthma action plan, often 4–10 puffs for an attack. Follow local emergency guidance if symptoms do not improve.
Mastering inhaler technique ensures faster symptom relief and can reduce escalation. The next section will cover when persistent or worsening signs such as increasing breathlessness, inability to speak in short sentences, or cyanosis require urgent ambulance activation.
Get CPR Certified in Minutes for as low as $19.95
Join thousands of professionals that have been certified online with us
Severe shortness of breath or barely moving chest.
Silent or very faint wheeze.
Blue/grey lips or face.
Unable to speak full sentences.
Sudden collapse or unresponsiveness.
While waiting for help, keep the person sitting upright to ease breathing. Administer the reliever inhaler using a spacer, giving 4–10 puffs one at a time, based on the National Asthma Council Australia guidelines. Continue to monitor their breathing and level of consciousness until emergency services arrive.
How can I reduce the risk of future attacks and stay prepared?
To reduce the risk of future attacks and stay prepares, follow a written asthma action plan, take preventer medication daily, avoid triggers, get the flu vaccine annually, and keep an emergency inhaler and spacer accessible at all times. Review your plan yearly or after a severe attack.
Can overuse of a reliever inhaler be dangerous?
Yes. Using a reliever more than 3 times a week (outside of emergencies) may signal poor asthma control and increased attack risk. Seek a medical review if frequent use is needed.
Can stress or strong emotions cause an asthma attack?
Yes. Emotional stress can trigger breathing difficulty in some people. Relaxation techniques and stress management may help reduce this risk.
Can drinking water help during an asthma attack?
Water may ease mild throat irritation, but it doesn’t relieve airway constriction. Always use your reliever inhaler and call for medical help if symptoms are serious.
Can asthma symptoms mimic a panic attack?
Yes. Shortness of breath, chest tightness, and rapid breathing occur in both. If inhaler use improves symptoms, it's likely asthma. If not, consider anxiety and seek help.
Why Should You Get Trained in First Aid?
You should get first aid training because it prepares you to act quickly in breathing emergencies like asthma attacks. It helps you recognize danger signs, use inhalers and spacers correctly, and give CPR if needed. CPR Select First Aid Training offers structured programs that build confidence, support care for vulnerable groups, and help maintain readiness through regular refreshers every 1–2 years. This ensures competence, prevents skill decay, and leads to better outcomes compared to relying on informal knowledge.



.avif)
.avif)